 One of the main alleged "official" nutrient recommendations for Pyrrole Disorder is vitamin B6, and the typical practitioner recommendation is to take vitamin B6 as pyridoxine hydrochloride (the inactive form) and P5P being the active form of this vitamin.
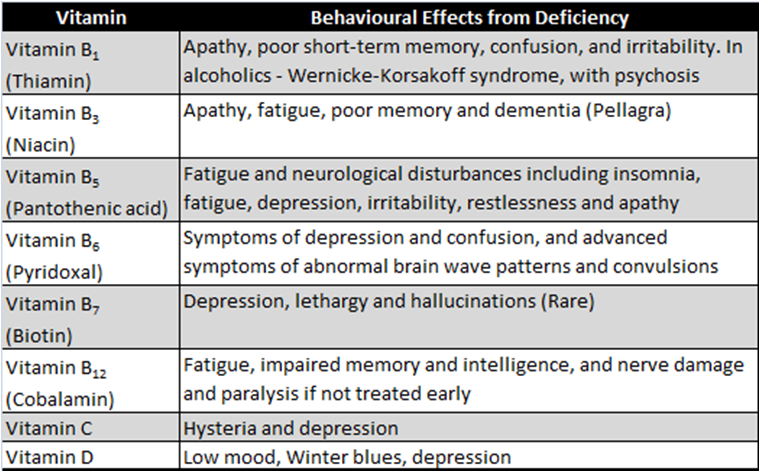
However, I do not recommend this... Some years ago I read some published studies which found that taking the inactive form (pyridoxine hydrochloride) together with P5P caused the inactive form to inhibit the body's use of the P5P - the main one your body can use! The pyridoxine hydrochloride form of B6 is also linked to causing peripheral neuropathy or nerve damage, which can cause symptoms of numbness or tingling in the extremities, loss of sensation, and also poor muscle control. This happens because of a deficiency of vitamin B6, but also in people who show very high levels of B6 in blood tests. This is likely as the body isn't able to use the B6, and causing the increasingly high levels on blood test, but at the same time as causing a functional deficiency of this vitamin and hence the deficiency symptoms. This neuropathy can take 2-3 months to start to develop after taking many of the usual compounded Pyrrole Primer or similar supplement products which are high in pyridoxine hydrochloride. Another reason why I don't recommend just taking B6 on its own, is that all the B-vitamins work together in many different biochemical pathways and reactions. Taking just one in a supplement may temporarily address that deficiency, but will quickly cause imbalances in the other Bs, to cause more symptoms. I believe these factors are why most people on the usual Primer or supplement protocols may get some initial improvements, but then plateau or collapse with the same or worse symptoms they had before taking the products. Every single case of a new Pyrrole Disorder client that comes to me, has a vitamin B12 deficiency, and over 50% have a vitamin B9 (Folate) deficiency too. Other B-vitamin deficiencies can also cause the common mental health symptoms and conditions seen in Pyrrole Disorder, as seen in the attached table. Again why those with this condition need ALL of the B-vitamins in a B-complex p just not necessarily a methylated B-complex, as many with this condition can be quite sensitive to the methylated forms of the Bs. But that's not in the official Walsh guidelines... another reason why I think they are wrong, and why I treat this condition differently.
0 Comments
 The generally recognised and recommended test for Pyrrole Disorder is the HPL urine test. However, I haven't used or recommended this test for a number of years because of the following reasons:
Hence why I recommend all of these additional tests as standard, to more holistically test for Pyrrole Disorder and its common related symptoms and conditions:
More important to getting these tests done is to make sure that you get an accurate analysis and interpretation of your results, as perhaps surprisingly, 99% of doctors (or other practitioners) do not interpret pathology results well. Pathology analysis is an area of specialty that I do, after training over 900 other practitioners on this skill. More information on why doctors don't analyse blood tests properly can be explained here: https://www.pathologyanalysis.com/pathology.html 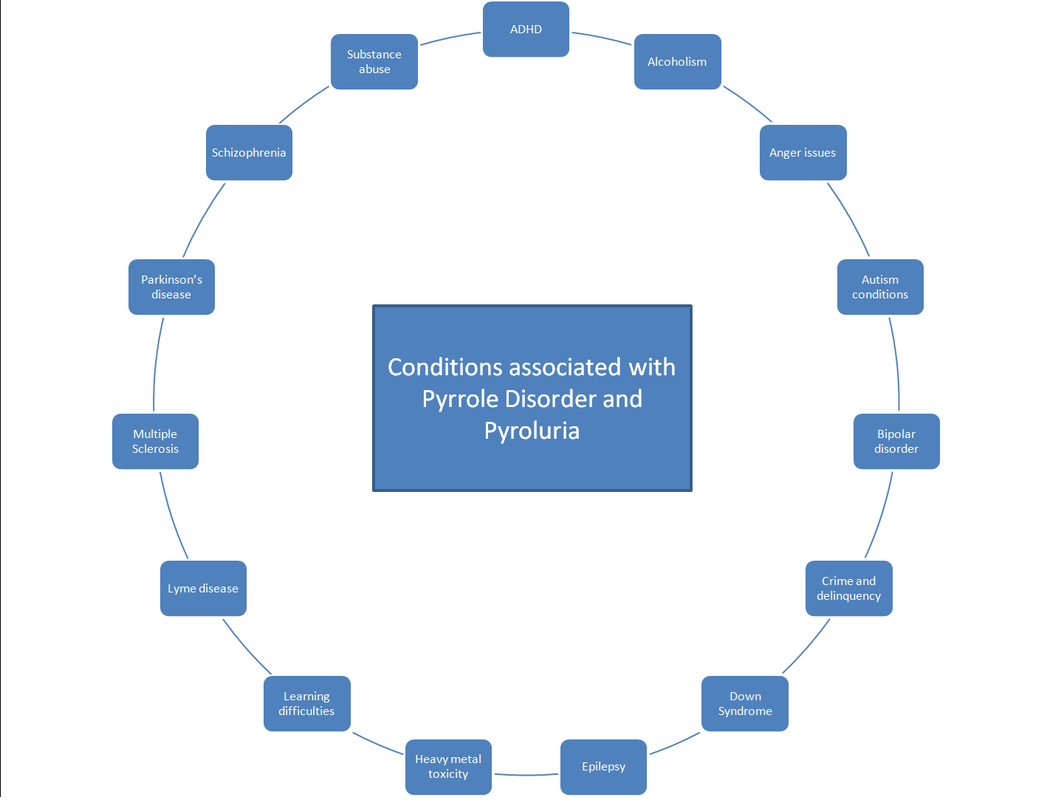 The excess production of the "pyrrole" compound in the body, and the nutrient deficiencies and metabolic or biochemical dysfunctions of Pyrrole Disorder, are known to cause many symptoms and conditions.
There are many other conditions which are commonly found in those with Pyrrole Disorder which are not as well known, but can be caused by and/or associated with PD or having elevated pyrrole compounds (HPL) in the urine, including all those shown in the attached diagram. Some of these conditions may be a surprise to some, including Lyme disease, Parkinson's disease, and the Autism spectrum disorders, especially ADHD, and more. I have seen many similarities of ADHD with Pyrrole Disorder, or many people being diagnosed with ADHD as well as Pyrrole Disorder, suggesting that they are perhaps one and the same condition. This information and graphic was based on a published scientific article on the pyrrole compounds being found in 80% of patients with chronic Lyme disease (Forsgren, 2009) and these other conditions too. This gives some hope and additional treatment options for people with Lyme disease, ADHD, and other conditions shown in the graphic. Reference: Forsgren, S. (2009). Kryptopyrroluria (aka Hemopyrrollactaminuria): A major piece of the puzzle in overcoming chronic Lyme Disease. Explore, 18 (6), 1-7.  Methylation is a biochemical process (involving chemistry of compounds and chemical reactions) involving the transfer of a methyl group (one carbon atom connected to 3 hydrogen atoms, or -CH3) to another chemical compound, for activation of the resulting compound or to cause some action. Of more relevance to health in general, methylation is also used for gene expression - methylation turns on or off the genes which can affect your health. This is called epigenetics - how your environmental factors turn on or off genes, without affecting the DNA underneath. For example, stress, your diet (and deficiencies), chemicals and toxins, lifestyle factors, sleep, etc, will either turn on or off genes to improve your health or to cause symptoms. With regard to Pyrrole Disorder, there is a belief that people with this condition are categorised into being an overmethylator or undermethylator, to explain how well (or not) the many body methylation processes are occuring. Some practitioners use a questionnaire of symptoms to determine if someone is one or the other, but I've never seen someone who has just symptoms of under vs over, so I question how true this classification really is. Other practitioners test histamine levels as a marker of over vs under, and others use different testing - there is no gold standard. Some genetic testing of genes such as MTHFR and others are sometimes used to check for methylation status too. Vitamin B12 and folate in your diet are methylation factors and do affect methylation, but should be taken into account for assessing methylation status, but these are typically not used for some strange reason. Many other nutrients are needed for methylation, or their deficiencies can affect methylation too. 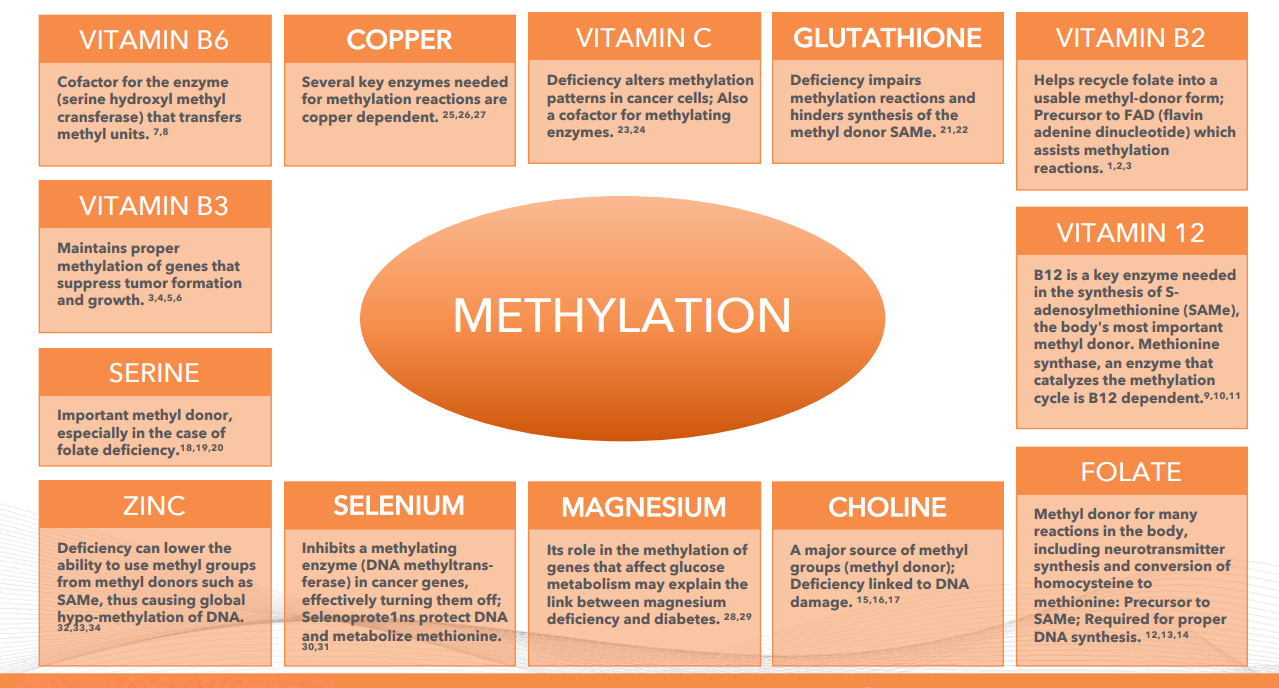 The thyroid function of controlling your metabolic rate will also affect methylation, and typically isn't taken into account either! I seriously question this methylation classification and I do not feel it is relevant for health in general or for pyrrole disorder. I do not believe that EVERY chemical process of methylation in the body is somehow running under or over! Some will likely be under and some being overmethylating and this will regularly change, because of many factors, hence why people with pyrroles have symptoms of both! In undermethylated people, the problem is usually due to a lack of methyl group production in methylation pathways from the abovementioned causes. It actually isn't possible to be an overmethylator as methyl groups and donors are available, but the cells or processes cannot actually use them, leading to high methyl levels hence the term "overmethylation", but causing a functional deficiency of methylation and LOW methylation symptoms. Hence "overmethylation" is just UNDERmethylation but having high availability of methyl groups. Hence don't worry about your alleged methylation status!  What is Pyrrole Disorder? It is a little known condition which can be initiated from severe or chronic stress or emotional trauma, which then triggers a genetic predisposition for excess production of a compound called HPL, which causes nutrient deficiencies. Because food nutrients are needed for a lot of functions and processes in your body, a deficiency in more than one nutrient will cause many seemingly separate symptoms. Specific nutrient deficiencies cause symptoms which result in Pyrrole Disorder (PD). Many GPs and doctors don't know about or recognise PD, as it just looks like you have a bunch of fairly common symptoms, including:
Pyrroles is nothing to be worried about! If anything it is great to have this diagnosis, as it is very easily treatable mainly with nutritional medicine! I've seen the condition in children as well as adults over 60 years of age, and it's always a relief to finally have an answer to their health issues! Pyrroles causes nutritional deficiencies mainly in zinc and vitamin B6, but also of lesser deficiencies in other B-vitamins, magnesium, omega-6 fats and others. Multiple deficiencies lead to all of the symptoms above, and more. Pyrroles is very frequently seen running in families across multiple generations. It is VERY common in those with Irish and Celtic family history, and the reasons for this are unknown. Some research shows that PD itself is very commonly linked to, and probably even a cause of bipolar disorder, schizophrenia, some autism disorders and other neurological and behavioural conditions. If you recognise many of the above symptoms (in the picture) in yourself, your children, or other people you know, it would be a good idea to see if Pyrroles may be the cause! I have seen substantial reductions of symptoms with the nutritional medicine treatment for this condition! And those who have improved feel like they have their life (and health) back again! |
AuthorWrite something about yourself. No need to be fancy, just an overview. Archives
March 2023
Categories
All
|
 RSS Feed
RSS Feed